Since the program was first enacted in 2014, Medicaid Expansion has helped provide access to health services for more than 219,000 Granite Staters. New Hampshire adults with low incomes, who may not be able to afford health insurance or may not have it provided through their employer, can enroll in health coverage that is almost entirely funded by the federal government. In the last fiscal year alone, more than 100,000 Granite Staters had access to health care through Medicaid Expansion at some point, bringing $502 million in federal dollars into the state. At the end of December 2022, more than 94,000 people were enrolled in the program.
Medicaid Expansion has helped ensure many more New Hampshire residents have had access to health care by enrolling people who could not otherwise afford or obtain coverage. In the five years following the implementation of Medicaid Expansion in New Hampshire, the number of Granite Staters lacking health coverage declined by approximately 58,000 residents, or 42.3 percent, relative to the five years prior to implementation. Available data suggest that, prior to the pandemic, many enrollees in Medicaid Expansion were likely to be on the program for relatively short periods of time, as transitional or seasonal losses in employment income made residents eligible for Medicaid Expansion until other work or health coverage opportunities arose. Temporary pandemic-era policies have enhanced access to eligibility since March 2020.
Medicaid Expansion has been particularly important for Granite Staters in need of mental health care, substance use disorder services, emergency room visits, and pharmacy services. Nearly 30,000 Granite Staters accessed mental health medication treatments at least once through Medicaid Expansion in the last fiscal year, while at least 8,600 unique individuals received some form of substance use disorder care services. Enrollees also relied on Medicaid Expansion for health needs during the pandemic, with more than 29,000 receiving care related to COVID-19. Additionally, more than 25,600 had at least one emergency department visit funded through Medicaid Expansion, and 792 received maternity care.
Younger adults are disproportionately likely to be enrolled in Medicaid Expansion relative to other age groups. Rural counties, and particularly counties that are more dependent on seasonal tourism, also have higher levels of enrollment. Available data suggests Granite Staters identifying as Hispanic, as Black or African American, as Native American, or as two or more races are disproportionately likely to have health coverage through Medicaid Expansion.
National and multistate research shows Medicaid Expansion is associated with enhanced access to coverage and key positive health outcomes. Reduced mortality and food insecurity, enhanced cancer detection, and improvements in birth outcomes have all been associated with Medicaid Expansion. Furthermore, improvements in household finances for enrollees contributed to reductions in evictions and medical debt. State economies overall also benefitted from Medicaid Expansion, with an infusion of federal resources contributing to boosts in employment and income, providing help for rural hospital finances, and enabling enrollees to more easily look for work or continue working.
New Hampshire funds the non-federal portion of Medicaid Expansion through a collection of taxes or assessments on insurance companies, revenue generated by the State’s liquor stores, contributions from a fund designed to help address alcohol abuse, a tax on hospital services, and any savings generated while operating the program. Medicaid Expansion also generates savings in the State Budget by offsetting other State costs, including payments for care to the uninsured at hospitals, Medicaid expenses with less favorable federal matching fund rates, and State medical expenses for incarcerated people. Other states that have comprehensively reviewed their Medicaid Expansion programs have found significant cost offsets, including some states that have found spending and revenue changes have completely offset the costs of Medicaid Expansion to their state budgets.
This Issue Brief reviews the impacts of Medicaid Expansion on health coverage for Granite Staters and the funding mechanisms used to support this coverage in New Hampshire. This Brief also analyzes research at the national level and from other states regarding the health, budgetary, and economic impacts of Medicaid Expansion.
Medicaid Expansion Program and Enrollment History in New Hampshire
Medicaid Expansion has substantially reduced the uninsured rate among Granite Staters, increasing access to critical health services for people with low incomes. This coverage provided vital health care access both before and during the pandemic.
Medicaid Expansion refers to the option states have to extend Medicaid coverage to adults with low incomes under the Patient Protection and Affordable Care Act. Specifically, adults aged 19 to 64 years with incomes below 138 percent of the federal poverty guidelines become eligible for health coverage under Medicaid Expansion.[1] In 2022, 138 percent of the federal poverty guidelines was the equivalent of $18,754 per year for an individual, or $31,781 for a family of three.[2] Estimates from 2021 suggest approximately 137,800 Granite Staters had incomes below 138 percent of the federal poverty threshold that year.[3] Other parts of the Medicaid program have lower income limits for coverage that is available only to adults with children, or cover people with disabilities or in other specific, qualifying situations.[4]
In New Hampshire, the Medicaid Expansion program was called the New Hampshire Health Protection Program at its initiation in August 2014, when it was authorized for a two-year period.[5] The program retained that name in New Hampshire when it was reauthorized in 2016 for another two years.[6] In January 2019, the Medicaid Expansion program was renamed to the New Hampshire Granite Advantage Health Care Program for a five-year reauthorization, which is in effect until December 31, 2023.[7] As part of the most recent reauthorization, services for most enrollees were reformed from being delivered through the Premium Assistance Program, which helped people pay for health insurance on the individual marketplace, to the privately-owned managed care organizations that contract with the State to administer key components of Medicaid coverage.[8]
Enrollment and Granite Staters served by Medicaid Expansion
Not long after implementation, enrollment in Medicaid Expansion began to climb, and many Granite Staters began to make temporary use of the program to access health services. Medicaid Expansion was first implemented in New Hampshire in August 2014, and by early December 2016, the number of enrollees had risen to about 51,500 Granite Staters. At that time, a total of 107,430 unique individuals had been enrolled at any one point in time since the program’s inception.[9] Only a year later, on November 28, 2017, the number of unique individuals served had risen to about 130,900, while program enrollment remained at about 52,000 residents at that time.[10] At the end of December 2022, 94,492 people were enrolled in the program.[11] From the start of the program in August 2014 through November 2022, 219,453 unique individuals had health coverage through Medicaid Expansion at some point in time.[12]
The high level of turnover in enrollment likely reflects both the flexibility of the Medicaid Expansion program and the employment opportunities for the people that rely on it the most for access to health care. As the key determinants of eligibility are income and age, Medicaid Expansion is quite responsive to changes in employment; Granite Staters who lose their jobs, and with it their income and any employer-covered insurance, may be able to enroll in Medicaid Expansion to retain health coverage.[13] Additionally, workers in jobs offering lower wages are more likely to face irregular, unpredictable, or unstable work hours, and may rely more on seasonal employment.[14] Turnover is also relatively high in key lower-wage industries in New Hampshire, including retail trade, the state’s second-largest employment sector, and accommodation and food services, the fourth-largest sector.[15]
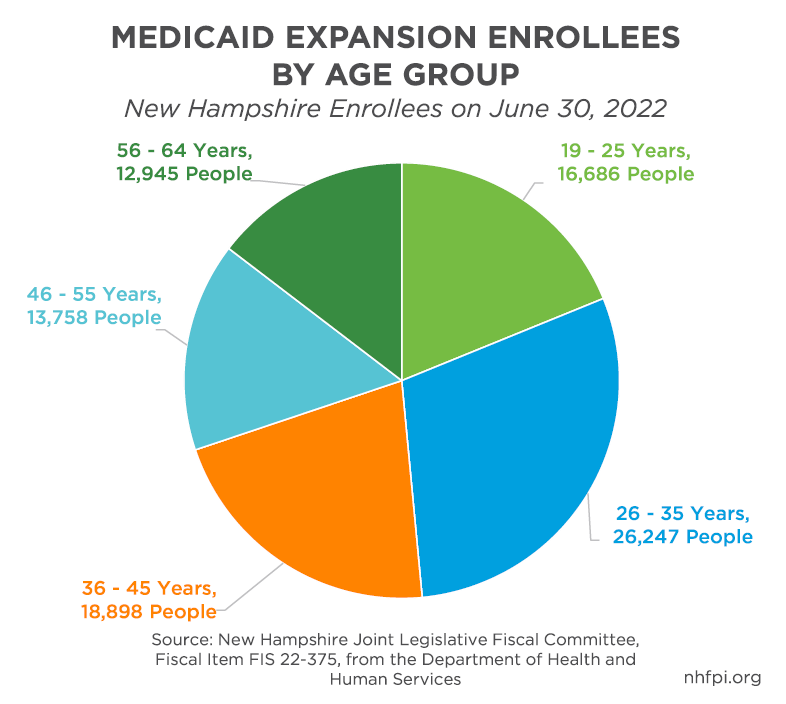
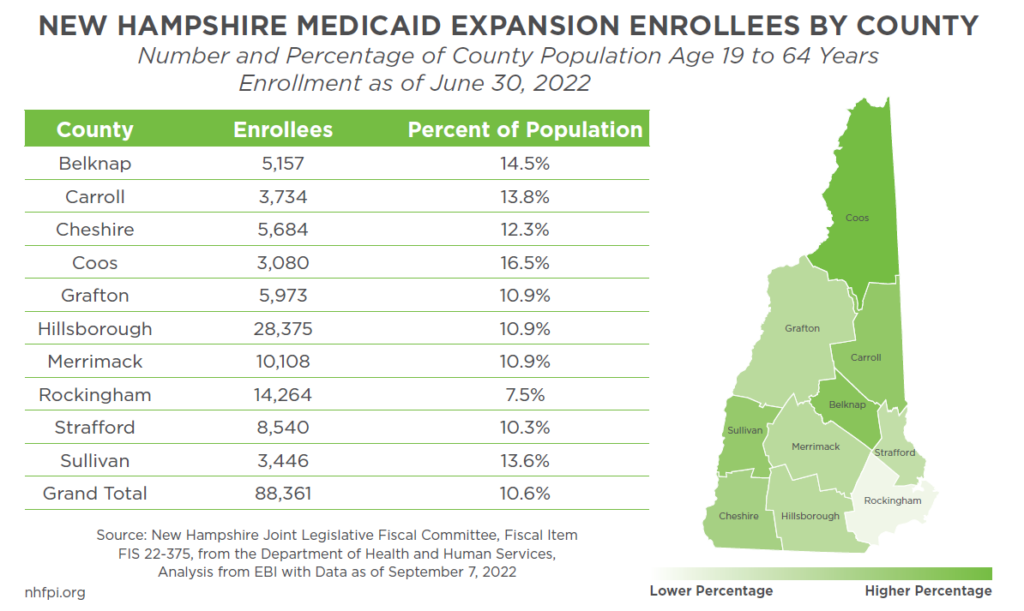
Other enrollment data provide insight into the population served as well, and reflect the likely importance of Medicaid Expansion to supporting workers with low incomes and in particular industries. At the end of June 2022, 26,247 enrollees, comprising 29.2 percent of all enrollees, were aged 25 to 34 years, which was substantially larger than older ten-year age groups. State-reported county-level enrollment also showed that rural areas with lower household incomes had higher percentages of their populations enrolled, particularly Coos (16.5 percent) and Sullivan (13.6 percent) counties. In Belknap and Carroll counties, which are more dependent on second homes or tourism and where retail trade or accommodation and food services are among the largest industries, enrollment in Medicaid Expansion was also relatively high, with both having about 14 percent of their populations enrolled in the program.[16] Of the 31 cities and towns in Hillsborough County, the state’s most populous, 8,971 enrollees lived outside of Manchester and Nashua as of August 1, 2022.[17]
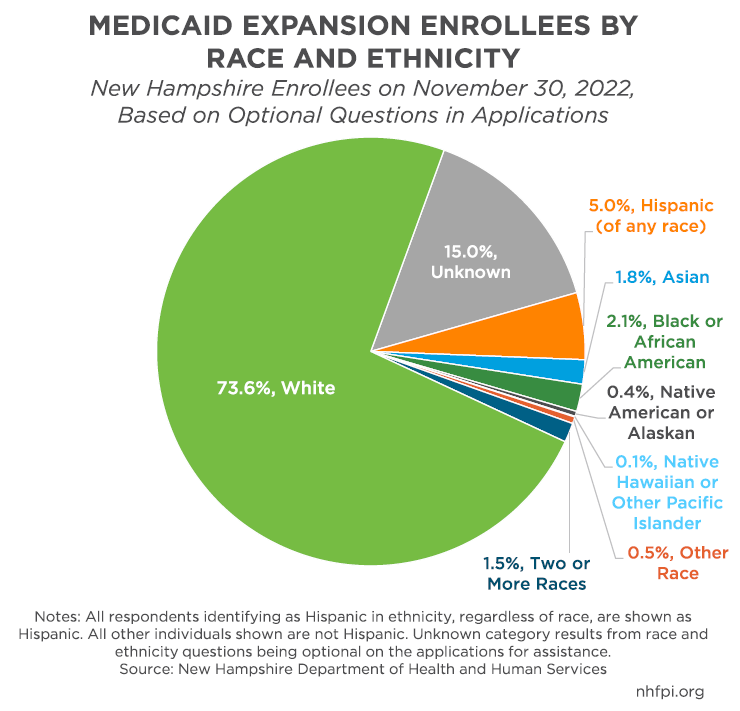
Individuals filling out applications for Medicaid Expansion also have the option of providing information about their race and ethnicity. While not all respondents did provide information, about 85 percent of enrollees on November 30, 2022 had information about their ethnicity, defined as identifying as Hispanic or not Hispanic, or race in the State’s files. Nearly three quarters of enrollees identified as white and not Hispanic, while 5 percent identified as Hispanic and of any race, and 2.1 percent identified as Black or African American and not Hispanic. Assuming the 15 percent of enrollees who did not report being Hispanic and did not provide a race were distributed proportionally among all the groups, people identifying as Hispanic, as Black or African American, as Native American, or as two or more races are disproportionately likely to be Medicaid Expansion enrollees relative to the overall population.[18]
While enrollment levels vary, Granite Staters in nearly every municipality in the state have access to health coverage through Medicaid Expansion. The Appendix of this Issue Brief lists the number of enrollees in each community and the aggregate expenditures deployed to provide those individuals with health care.
Increased Health Coverage and Access for Granite Staters
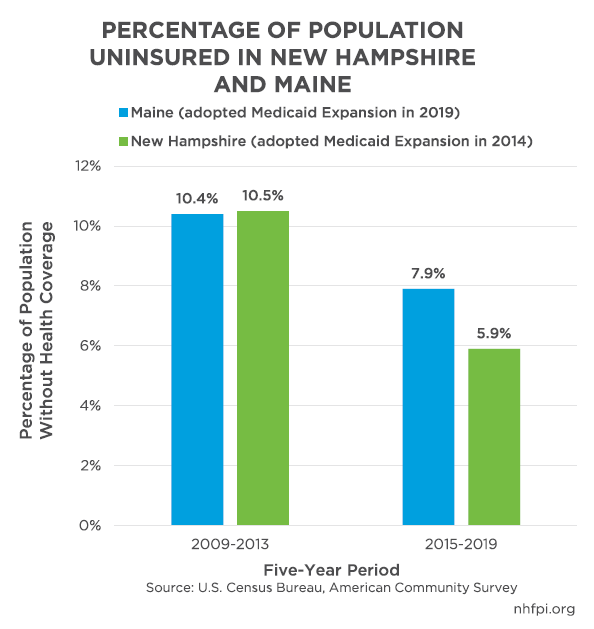
Following Medicaid Expansion’s implementation in 2014, fewer New Hampshire residents were uninsured. Averaged across the years 2009 to 2013, about 10.5 percent of New Hampshire’s civilian population did not have health insurance of any form. In the 2015-2019 period, following the implementation of Medicaid Expansion in August 2014, only 5.9 percent of Granite Staters were uninsured. The drop in the number of people uninsured in New Hampshire across these two periods was approximately 58,000 residents, or a 42.3 percent decline in the number of Granite Staters lacking health coverage.[19]
During the 2009-2013 period, the economy was slowly beginning to recover from the Great Recession. In contrast, the period from 2015-2019 included a more robust economic recovery, coinciding with a tight labor market and more income growth, including among workers with lower and median wages.[20] This higher rate of employment and income growth likely would have reduced the number of uninsured Granite Staters even if Medicaid Expansion had not been implemented. Neighboring Maine, however, did not adopt Medicaid Expansion until 2019, and New Hampshire’s uninsured rate dropped faster between these two periods than it did there. Maine’s uninsured rate in the 2009-2013 period was 10.4 percent, nearly identical to New Hampshire’s, but only fell 2.5 percentage points to 7.9 percent in the 2015-2019 period, compared to New Hampshire’s drop of 4.6 percentage points.[21]
Increased health care access was especially pronounced among certain groups of Granite Staters. While approximately 14.7 percent of Granite Staters aged 18 to 64 years old did not have health insurance prior to Medicaid Expansion, about 8.6 percent of 19-to-64-year-olds lacked coverage in the five years following the program’s implementation; while these age ranges do not exactly align, the data show a clear downward trend in the approximate age group eligible for Medicaid Expansion. More children also gained insurance coverage across these time periods. Additionally, while over one out of every five Granite Staters of any age with incomes below 138 percent of the federal poverty threshold lacked insurance in the five years before enactment, slightly more than one in ten did not have coverage in the five calendar years following Medicaid Expansion’s implementation. This change represents a 59.9 percent decrease in the number of people in or near poverty who lacked health coverage in New Hampshire. The uninsured rate for people in households with less than $50,000 in annual income fell 8.5 percentage points, while part-time or seasonal workers experienced a 7.4 percentage point decline.[22]
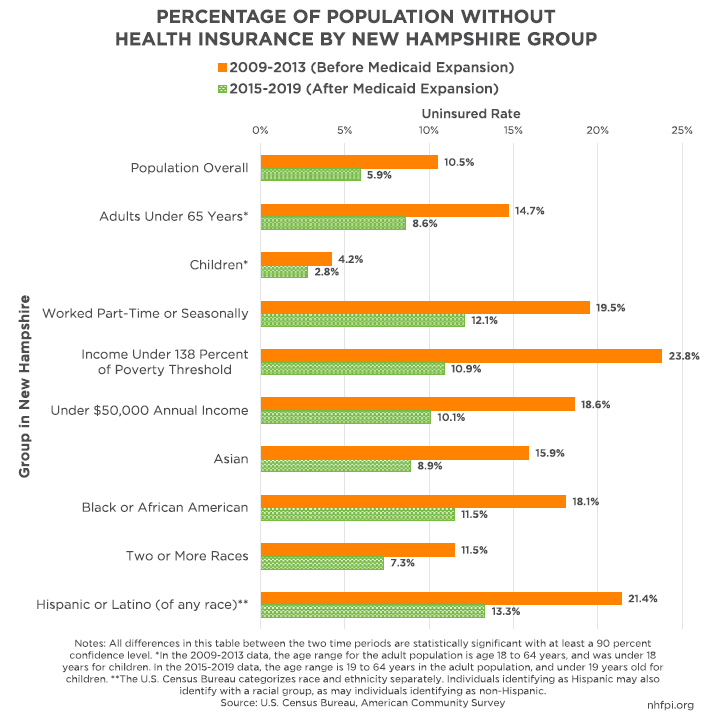
Significant drops in uninsured rates also occurred among ethnic and racial minority populations in New Hampshire. The percentage of Granite Staters identifying as Black or African American without health coverage dropped 6.6 percentage points, and the rate for New Hampshire residents identifying as Asian fell 7.0 percentage points. Granite Staters identifying as two or more races saw their uninsured rate fall 4.2 percent, and people of any race identifying as ethnically Hispanic or Latino experienced a decline of about 8.1 percentage points. Among the non-Hispanic white population, the uninsured rate dropped 4.5 percentage points.[23] National research shows that Medicaid Expansion has helped reduce differences in insurance rates and outcomes among racial and ethnic groups, and has also helped extend coverage to people with disabilities who may face difficulty qualifying for coverage through other components of Medicaid.[24] As described later in this Issue Brief, research also shows Medicaid Expansion programs are associated with increases in health coverage.
Coverage Expansion Enables Access to Key Health Care
As with prior years, Granite Staters enrolled in Medicaid Expansion had access to vital health services during State Fiscal Year (SFY) 2022, which lasted from July 1, 2021 to June 30, 2022. Using data available through the end of August 2022, the State reported that there were tens of thousands of unique individuals using different types of services funded through Medicaid Expansion during SFY 2022, including:[25]
- 29,941 people receiving mental health medication treatments
- 11,456 people receiving mental health outpatient services
- 6,228 people for an inpatient hospital visit or visits of any type
- 864 people with mental health inpatient hospital treatments
- 2,303 people with substance use disorder services via residential or inpatient hospital treatments
- 8,057 people with medication-assisted substance use disorder treatments
- 8,645 people with substance use disorder outpatient services
- 792 people receiving maternity care
- 25,606 people who had an emergency department visit or visits
- 17,849 people with preventive or well care visits
- 29,073 people receiving services related to COVID-19
- 63,734 people for whom payments were made for pharmacy services
Medicaid Expansion also paid for 6,000 people who needed dental care, including enrollees aged 19 and 20 years who had full dental benefits and enrollees aged 21 years and older who only had emergency dental services covered through Medicaid Expansion.[26]
These unique individuals accessing services may have needed some or all of the other types of services in this list as well, and may have accessed the same services, such as treatments or pharmacy services, multiple times.
As a later section of this Issue Brief reviews, research indicates Medicaid Expansion improves access to care and may help reduce mortality. Access to the care delivered to the people enumerated in the list above may have been much more limited without Medicaid Expansion.
Key Assistance During the COVID-19 Crisis
At the onset of the COVID-19 pandemic in the United States, the federal government responded with a wide variety of policies, including steps to help ensure people did not lose their health coverage.[27] During the ongoing federally-declared Public Health Emergency, states receive a 6.2 percent boost in the federal matching dollars supplied for most aspects of their Medicaid programs. Medicaid Expansion, however, did not receive this boost and remains at a 90 percent match. Paired with the increased Medicaid boost in funding for most of the program, the federal government has restricted the ability of states to disenroll individuals from Medicaid, including Medicaid Expansion, who were found eligible at some point during the Public Health Emergency. While this current continuous enrollment requirement will end on April 1, 2023, it has effectively kept many people enrolled in Medicaid who may have been determined to be ineligible and disenrolled under pre-pandemic rules.[28]
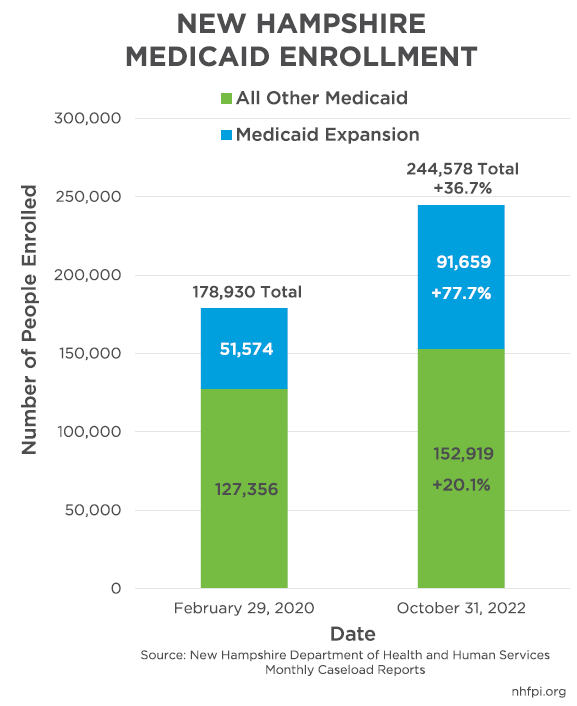
Since the continuous enrollment policy was adopted in early March 2020, Medicaid enrollment in New Hampshire has increased significantly. Overall Medicaid enrollment climbed by 65,648 between the end of February 2020 and the end of October 2022, a 36.7 percent increase. Medicaid Expansion contributed to 61.1 percent of this increase, with enrollment through Medicaid Expansion increasing by 77.7 percent, or 40,085 individuals.[29]
This climb in enrollment represents a significant number of Granite Staters who have relied on the program for access to health care, even relative to prior levels of turnover among enrollees. Medicaid Expansion has provided coverage at some point to 219,453 unique people in New Hampshire from its inception in August 2014 to the end of November 2022. From August 2014 through December 2019, 171,745 different individuals were served. Since the beginning of 2020, 122,688 unique Granite Staters have been enrolled in Medicaid Expansion at some point.[30]
A national-level May 2022 analysis of past and projected Medicaid expenses due to this rising enrollment and these enhanced federal revenues found that New Hampshire received slightly more in revenue from the federal government than the additional cost to the State to pay for higher Medicaid enrollment.[31] This suggests the federal government effectively covered the added expenses from those enrollees.
When more than 100,000 Granite Staters became unemployed, and many more residents lost employment income, in the initial months of the COVID-19 pandemic’s impacts in New Hampshire, Medicaid Expansion served as a key way to maintain access to medical care during this public health crisis.[32]
Continuous enrollment helped ensure that individuals and families whose finances were damaged by the pandemic could still maintain access to health care. This continuous access was particularly important given the diminished stability of employment in key sectors impacted by the pandemic, such as accommodation and food services. The federal Public Health Emergency is still in effect, and as of September 6, 2022, 43,566 Medicaid Expansion enrollees have not provided the State with sufficient information to determine their eligibility after the Public Health Emergency ends. These individuals are at risk of losing health coverage, as a recently-enacted federal statute will end Medicaid’s continuous enrollment provisions on April 1, 2023, when enrollment redeterminations will resume and federal funding will begin to decrease. The State expects enrollment to decline significantly after the continuous enrollment provisions expire.[33]
Positive Effects on Health Coverage for Children
While coverage through Medicaid Expansion is for adults aged 19 to 64, children can indirectly benefit from Medicaid Expansion. Adults with low incomes who access Medicaid Expansion are more likely to enroll their children in Medicaid. Typically, Medicaid for children has higher income eligibility thresholds than adults due to the federal Children’s Health Insurance Program, which is a component of broader Medicaid programming in many states, including New Hampshire.[34]
Expansions in health coverage to adults spurred greater enrollment for previously-eligible children. One Health Affairs study identified Medicaid enrollment increases between 2013 and 2015 for children of parents who received coverage under Medicaid Expansion in their states. Those increases were approximately twice as large, in percentage terms, than the increases for children with parents who were not newly eligible under Medicaid Expansion due to living in states without it.[35] Other research found an approximately 29 percent increase in the likelihood a child completes an annual child wellness visit, a preventive care service, if that child’s parents are enrolled in Medicaid.[36]
In New Hampshire, of the 91,507 enrollees in Medicaid Expansion on October 1, 2022, 25,931 (28.3 percent) had children under the age of 18 years in their household. Among those enrollees with children, 10,255 had kids under the age of five years.[37]
Funding Medicaid Expansion in New Hamsphire
Medicaid Expansion represents a significant investment in the health of Granite Staters. In SFY 2022, the total cost of Medicaid Expansion was about $558.2 million. These funds provided access to health coverage for 100,980 unique individuals, with 90 percent of the cost covered by the federal government.[38] The SFY 2022 Medicaid Expansion expenditure total was a substantial increase from pre-pandemic levels, which were $492.2 million in SFY 2018 and only $382.3 million in SFY 2020.[39]
The lower figure in SFY 2020, despite the onset of the COVID-19 pandemic in the last third of the year, was in part due to cost-saving reforms to the program that were implemented halfway through SFY 2019. This reform eliminated the Premium Assistance Program under the New Hampshire Health Protection Program, shifting all Medicaid Expansion enrollees, including those previously receiving premium payment assistance on the individual exchanges, to the managed care organizations; the entire program was renamed the New Hampshire Granite Advantage Health Care Program.[40]
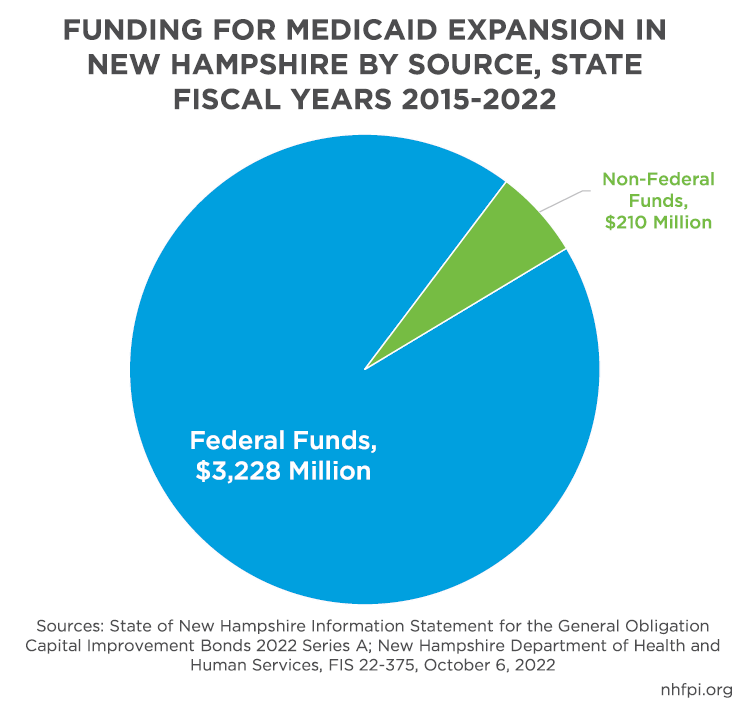
Since the Medicaid Expansion program began in New Hampshire, approximately 93.9 percent of funding has come from the federal government. This percentage is higher than 90 percent because the federal government paid for the entire cost of the program in calendar years 2014 to 2016, and the match rate declined incrementally to 90 percent between 2017 and 2020. The 90 percent match is set by statute to continue permanently. In total, about $3.228 billion in federal funds and $210 million in non-federal funds have paid for the program in New Hampshire from August 1, 2014 through June 30, 2022.[41]
Funding the Non-federal Share in New Hampshire
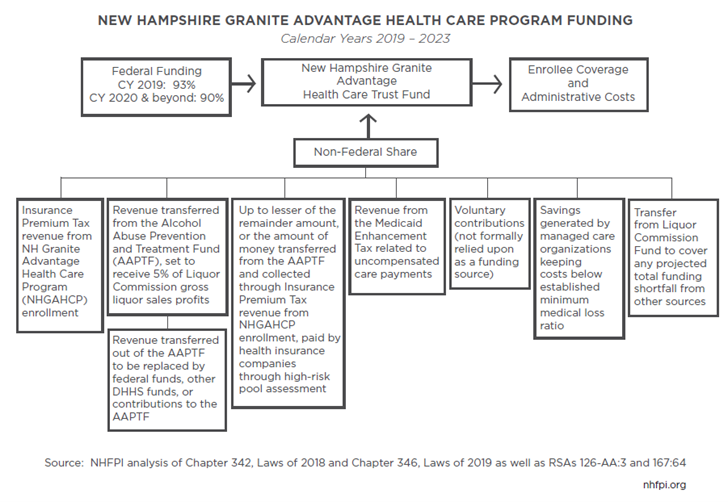
While the federal government funded more than $502 million of the total cost of Medicaid Expansion in SFY 2022, the State was responsible for raising the remaining $56.2 million, or about 10 percent of total costs, including administrative expenses.[42]
During the last four years, New Hampshire has relied on a variety of revenue sources to raise these funds annually, including:[43]
- Insurance Premium Tax revenues generated in association with Medicaid Expansion
- An assessment on health insurance providers previously associated with a high-risk pool of enrollees
- Revenue transferred from the Alcohol Abuse Prevention and Treatment Fund
- A portion of Medicaid Enhancement Tax revenues associated with uncompensated care cost calculations at hospitals in the state and other payments made to those hospitals
- Voluntary contributions made to the New Hampshire Granite Advantage Health Care Trust Fund
- Any savings generated due to the State-contracted managed care organizations keeping program costs below established minimum medical loss ratios
- Funds drawn from the Liquor Commission Fund to cover any shortfall remaining after the contributions of all the revenue sources listed above
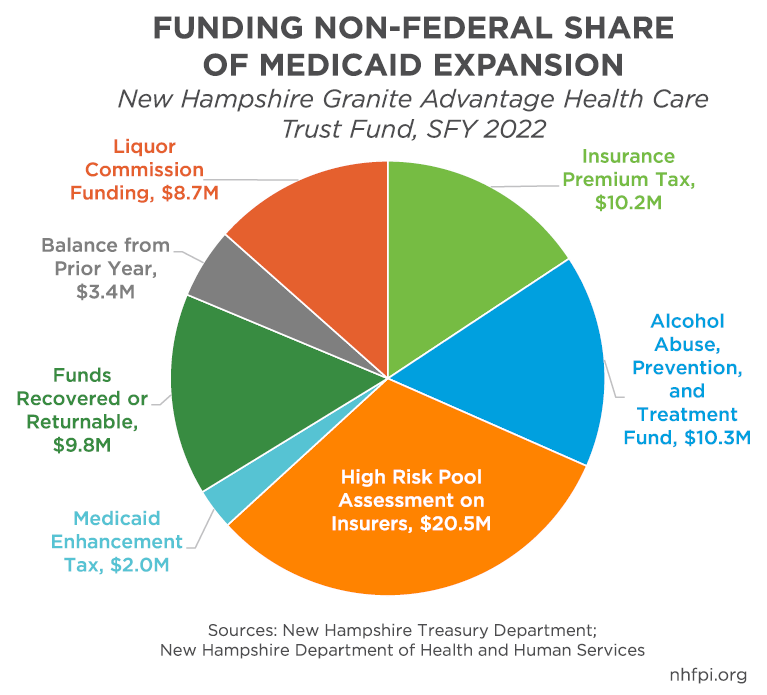
The most significant of these funding sources are the high risk pool assessment on insurers, the funding transferred from the Alcohol Abuse Prevention and Treatment Fund, and the Insurance Premium Tax revenues.[44] The Liquor Commission Fund was added as a revenue source to State law in September 2019 to help ensure the program never faced a revenue shortfall that would have otherwise triggered the end of the program. In SFYs 2021 and 2022, the program utilized $8.5 million and $8.7 million of Liquor Commission Fund revenues, respectively, to provide health coverage during the COVID-19 pandemic.[45]
While federal funds are matched with State General Funds to fund health services in most other components of the State’s Medicaid program, State law prohibits Medicaid Expansion’s non-federal share from being funded by General Funds.[46] The General Fund holds the resources that are the most flexible for State policymakers to use, and are primarily generated by State taxes.[47]
Key Cost Savings from Medicaid Expansion
In New Hampshire, Medicaid Expansion is funded entirely outside the State Budget, but it does interact with State Budget expenditures.[48] Although no General Fund expenditures are used directly to fund Medicaid Expansion, the State may experience General Fund savings because federal funds through Medicaid Expansion can offset expenditures that would have been financed through General Funds.
While 90 percent of Medicaid Expansion’s funding is from the federal government, most other components of Medicaid are only 50 percent funded by federal transfers.[49] As a result, adults age 19 to 64 who might be enrolled in other parts of Medicaid, including parents with very low incomes, pregnant women, or individuals who may qualify because of a disability, would likely have half of their health care needs funded by General Funds.[50] When individuals eligible for both traditional Medicaid and Medicaid Expansion are enrolled in Medicaid Expansion, no General Funds are used directly, and the State only pays for 10 percent of coverage costs while the federal government covers 90 percent.
The State also funds payments, called Disproportionate Share Payments, to hospitals for the costs of uncompensated care provided to uninsured residents. In SFY 2021, the State paid $193.1 million in Disproportionate Share Payments, about half of which was federal dollars while the rest was generated by the State, including through the Medicaid Enhancement Tax.[51] While several factors affect the amount of the Disproportionate Share Payments, and uncompensated care costs associated with caring for Medicaid enrollees have risen, hospitals have seen lower costs associated with uncompensated care for uninsured patients since Medicaid Expansion was enacted. The New Hampshire Hospital Association reports uncompensated care costs associated with people who were uninsured averaged $157.0 million across SFYs 2012-2014, but fell to $65.1 million in SFYs 2017-2019, after Medicaid Expansion’s implementation and before the COVID-19 pandemic.[52] While reimbursements are made for certain Medicaid enrollee care costs, reducing the number of people who are uninsured helps to limit the costs and need for payments based on uncompensated care to the uninsured made by the State.
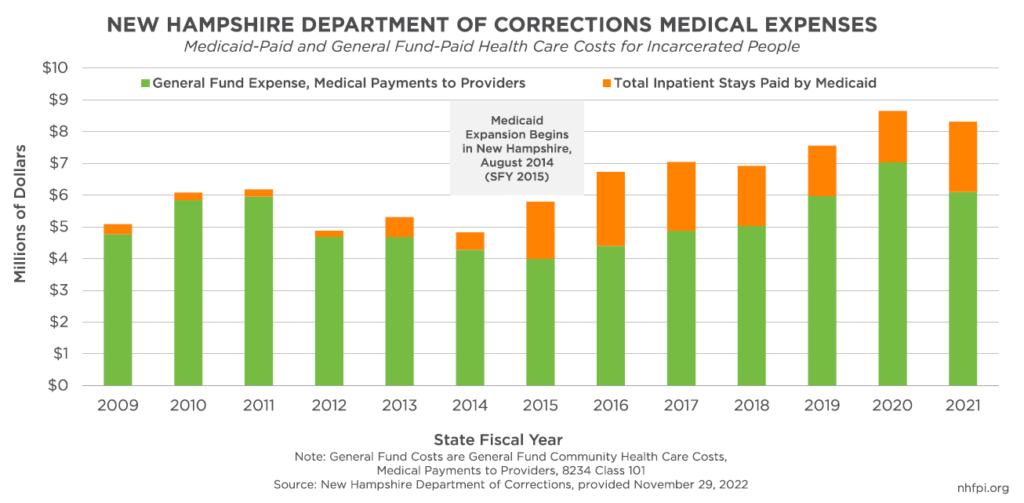
General Fund savings can also be generated because of lower costs in other areas, including fewer needs for other services. For example, the Department of Corrections pays for certain community medical costs for incarcerated residents. In the six years prior to the implementation of Medicaid Expansion, from SFYs 2009 through 2014, Medicaid paid an average of $359,186 (6.7 percent) of these health care costs each year. In the six full years after the implementation of Medicaid Expansion, the average dollar value of Department of Corrections community medical costs covered by Medicaid rose to $2.0 million annually, totaling 26.1 percent of all these expenses from SFYs 2016 through 2021.[53] If the percentage of total community medical costs for incarcerated residents had remained at the pre-Medicaid Expansion average of 6.7 percent, General Fund expenses would have been $10.2 million higher from SFYs 2015 to 2021.
Medicaid Expansion Savings in Other States
Several state-level and national analyses have sought to understand the aggregate impact of adopting Medicaid Expansion on state budgets and finances. Overall, there appears to be a high potential for savings in other areas of state expenditures and increased tax revenues to largely, if not completely, offset the fiscal costs to states of Medicaid Expansion, with varying experiences dependent on the particular state.
Medicaid Expansion appears to have generated significant savings in other parts of state Medicaid programs. Analysis from The Commonwealth Fund found that, between federal fiscal years 2014 and 2017, states with Medicaid Expansion had more than 4 percent savings in their traditional Medicaid programs relative to states without Medicaid Expansion. Across SFYs 2015-2019, states undertaking Medicaid Expansion did not see a statistically significant increase in non-federal expenditures, although the federal match rate was higher than 90 percent for Medicaid Expansion during these early years of the program.[54]
States that performed individual analyses of their total estimated savings resulting from Medicaid Expansion in their other Medicaid programs found widely varying amounts of offset. The Commonwealth Fund employed these individual analyses to project estimated savings to 2020. Of ten states that performed individual examinations used as the basis for these estimates, one (Ohio) found only 7 percent of the state share of Medicaid Expansion costs would be offset by savings elsewhere in Medicaid, and two more (Kentucky and Michigan) estimated 10 percent would be offset. All other states, however, estimated at least 46 percent of state Medicaid Expansion costs would be offset by these savings, including 85 percent in three states (Virginia, Colorado, and Washington).[55]
Some states also produced estimates of other savings, which were primarily generated in reduced spending on other, non-Medicaid mental health and substance abuse treatment programs, uncompensated care payments to providers, and health services for inmates at correctional facilities.[56] Savings in these areas varied widely, and were dependent on the structures of other programs within the states, but savings were estimated in all cases. One national study found that, between fiscal years 2013 and 2015, state corrections department health spending grew by 10 percent in states that did not adopt Medicaid Expansion, but only 4 percent in states that did implement the program.[57]
Four states with detailed analyses available and different policy approaches showed the substantial variation in the extent of savings, but all indicated Medicaid Expansion costs were substantially offset by savings. In Montana, combined estimated savings from Medicaid and other programs, increased hospital tax revenues and premiums, and more tax revenue generated by increased economic activity were estimated to barely, but fully, offset state Medicaid Expansion costs.[58] In Ohio, projections indicated the state would, after offsets, pay about 30 percent of the non-federal share of Medicaid Expansion, or about 3 percent of the entire program’s cost. Estimates from two different studies in Michigan, which is required to offset its Medicaid Expansion costs with identified savings, suggested that Michigan would have cost savings of about $180 million in SFY 2021, without including about $136 million in additional tax revenues generated from Medicaid Expansion-induced economic activity, for a total of 169 percent of state program costs paid for by offsets. Finally, in Virginia, policymakers expected savings in traditional Medicaid to only offset some of the state cost of Medicaid Expansion, but those projected savings were later updated after an unexpectedly large number of people switched from other parts of the Medicaid program to Medicaid Expansion, leading to a projected 141 percent of state costs covered by savings in SFY 2020; savings elsewhere in the State Budget were projected to save the equivalent of 17 percent of the state’s Medicaid Expansion costs.[59]
In a January 2022 analysis, The Hilltop Institute examined a potential Medicaid Expansion in Mississippi. This analysis projected that savings from Medicaid Expansion, including from increased direct and indirect tax revenues, would entirely offset additional state costs in 2023 and 2024, and generate a total of $27.6 million in state costs from 2025 to 2028, or about 3.5 percent of the estimated state costs before offsets and without federal matching funds.[60]
Health Effects of Medicaid Expansion
Medicaid Expansion enhances access to health services for adults with low incomes by removing or reducing the financial cost of accessing those services. This improved access means individuals may get treatment, either for existing ailments or preventative care, that they would not otherwise have received or been able to afford. The availability of this coverage also reduces financial burdens on individuals and families that otherwise would have been paying premiums for private insurance, been paying out of pocket, or passing some or all the costs of obtaining care on to providers.
In an effort to understand available research regarding the effects of Medicaid Expansion, the Kaiser Family Foundation conducted two literature reviews, published in early 2020 and in mid-2021, of 601 studies of the impact of state-level Medicaid Expansions published between January 2014 and March 2021. With some exceptions showing mixed or limited results, these studies generally found positive effects of Medicaid Expansion on different key outcomes, including access and utilization of care, enhanced health coverage, and improved financial stability, higher food security, reduced eviction risk, and lower medical debt for households.[61]
The Kaiser Family Foundation’s reviews found a growing body of research identifying Medicaid Expansion was associated with reduced overall mortality and mortality specifically associated with certain specific health conditions, including during pregnancy or childbirth and for certain types of cancer, cardiovascular disease, and liver disease. Medicaid Expansion increases health coverage and is associated with higher early-stage cancer diagnosis rates. Studies have also identified increased coverage before, during, and after the birth of a child associated with Medicaid Expansion, as well as improvements in birth outcomes like low birth weight. While the reviewed research has not conclusively determined whether Medicaid Expansion has led to a widespread reduction in infant mortality, a 2018 study found bigger declines in infant mortality between 2010 and 2016 in states with Medicaid Expansion compared to those without it.[62]
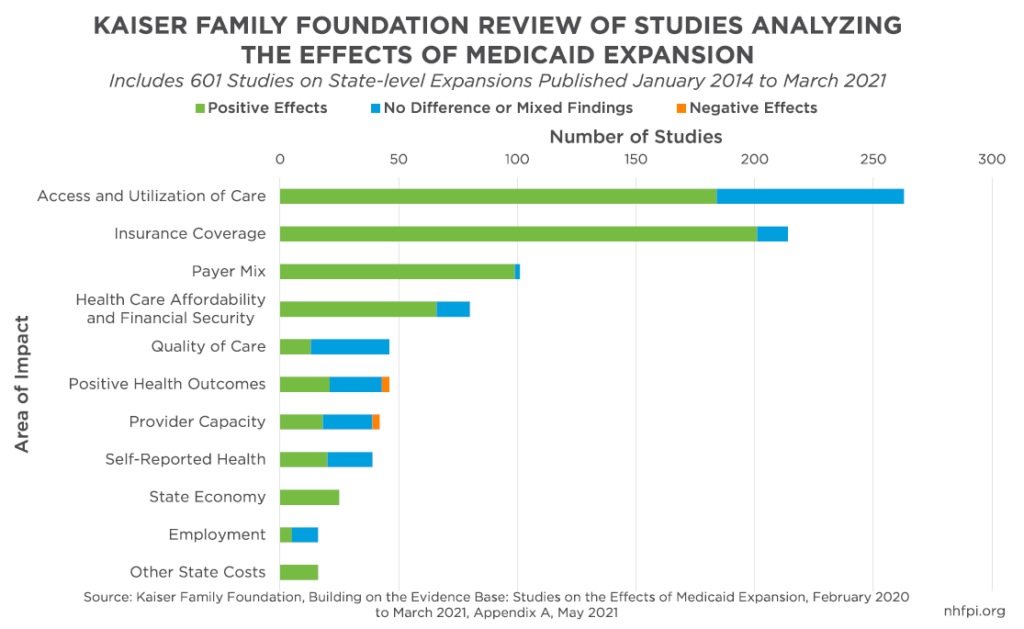
The review also found improvements in access to care, particularly among people with low incomes, people accessing substance use disorder services, and individuals with mental health needs. Measured impacts vary by study and population group. Some studies also reported Medicaid Expansion was associated with better self-reported health and more healthy behaviors, including around the management of diabetes.[63] While impacts on providers were also somewhat mixed in the studies examined, rural and small hospital finances appear to have been particularly bolstered by Medicaid Expansion, helping to stave off closures or reduced services at hospitals.[64]
Economic Benefits
Since Medicaid Expansion was first implemented in New Hampshire from August 2014 until June 2022, the program has brought nearly $3.23 billion in federal funds to New Hampshire, supporting the health of Granite Staters and the economy.[65] The New Hampshire Department of Health and Human Services projected another $561 million would come to the Granite State through the program in SFY 2023.[66] Like federal dollars for food assistance, unemployment benefits, and home heating aid, these funds support the local economy, including supporting key parts of the health care system, such as hospitals in rural areas.[67] Rural hospitals are often key for local economic activity; research indicates rural hospital closures are associated with declines in local employment, and may negatively impact labor force participation, regional population growth, and per capita income.[68] Additionally, positive health impacts and economic security associated with having health coverage may help individuals more fully engage in the economy and their communities.
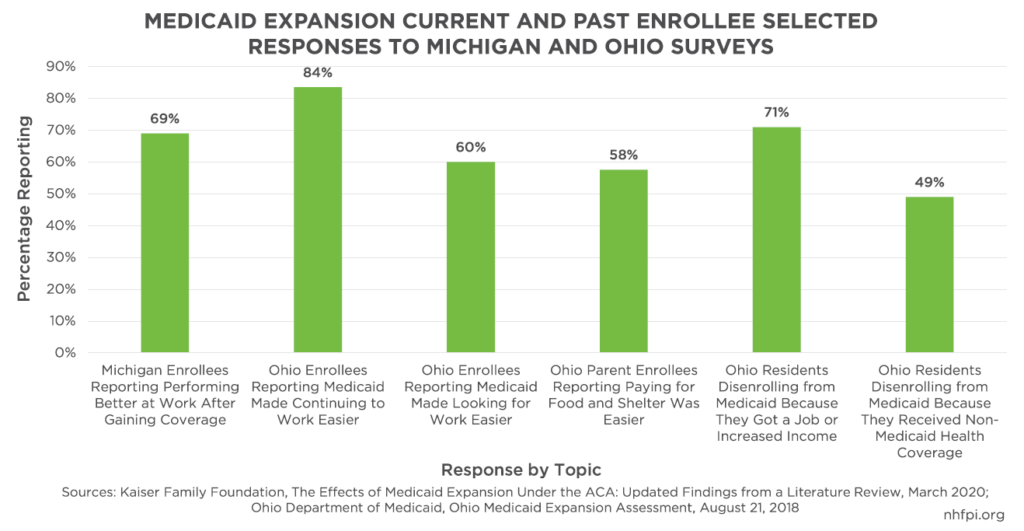
The Kaiser Family Foundation’s reviews of Medicaid Expansion research identified 25 studies focused on the overall effects on state economies, and all found positive impacts from Medicaid Expansion.[69] These benefits likely stem from both the direct impacts of a significant amount of federal resources entering the states‘ economies due to 90 percent of the cost of services being paid for by the federal government, and from Medicaid Expansion enhancing the ability of individuals to work. The review found that Medicaid Expansion was linked to overall increases in employment, and several studies found that Medicaid Expansion enrollees had enhanced abilities to work following their enrollment. This research included two separate surveys in Michigan that found 69 percent of Medicaid Expansion enrollees reported performing better at work once they had coverage through Medicaid Expansion, and 46 percent of Michigan primary care physicians surveyed reported Medicaid Expansion had a positive impact on patients’ abilities to work. Some studies found no impact on employee behavior from Medicaid Expansion, and only one found a negative effect on employment from Medicaid Expansion, but the effect was temporary and did not persist in the following year, nor did it have any impact on wages.[70]
A 2018 survey of Ohio enrollees and former enrollees published by the state government found nearly 84 percent of respondents reported Medicaid Expansion made it easier to continue working, and 60 percent reported Medicaid made looking for work easier. Of the people who unenrolled from Medicaid Expansion, 290,000 (or 71 percent of respondents) got a job or increased their income, and almost half of those who unenrolled did so because they obtained non-Medicaid health coverage, such as through employer-sponsored coverage.[71]
A 2021 analysis conducted by The Commonwealth Fund projected that, if the 14 states identified as not yet having implemented Medicaid Expansion had completed rollouts starting in 2022, more than a million new jobs across key economic sectors would have been created in 2022, including more jobs in each state that newly instituted Medicaid Expansion. Personal income would have been boosted in each state, with an aggregate increase of nearly a quarter of a trillion dollars nationwide during calendar years 2022 to 2025, relative to these states not adopting Medicaid Expansion.[72]
A more recent study, The Hilltop Institute’s 2022 analysis of the potential Medicaid Expansion in Mississippi, projected over 10,500 jobs would be generated and sustained by Medicaid Expansion in that state from 2023 to 2028. The study also projected more than $800 million in increased economic activity added to the Mississippi economy each year relative to the economy without Medicaid Expansion.[73]
Conclusion
Medicaid Expansion in New Hampshire has benefitted the states’ residents, particularly those who have been least able to afford health insurance. Since the program’s beginning in 2014, over $3.2 billion from the federal government has funded health care for Granite Staters, providing financial stability for households experiencing hard times and helping ensure access to doctors, hospitals, and treatments for mental health or substance use disorders. These dollars have also helped the economy, and made more resources available for key parts of the health care system, including front-line health care staff and rural hospitals.
Reductions in the uninsured population and enhancements to care access likely have a positive impact on health outcomes. With nearly 30,000 people receiving mental health treatments through Medicaid Expansion, and indications that adults enrolled in Medicaid are more likely to enroll their already-eligible children as well, the expanded coverage has a favorable impact on both families and the state’s workforce overall. The reductions in food insecurity, medical debt, and evictions associated with Medicaid Expansion could all have significant long-term benefits for individuals and families.
Although comprehensive data are not available for New Hampshire, research from other states suggests that the costs of Medicaid Expansion to state budgets, which accounts for only ten percent of the program’s total expenditures, are substantially offset by savings in other programs or enhanced tax revenues from boosts in economic activity. While some states estimated a net expenditure increase in their state budgets, others identified savings that more than covered the state’s Medicaid Expansion costs.
Medicaid Expansion provided a key support during the COVID-19 pandemic’s worst months, providing access to health care even during times of significant employment disruptions. However, Medicaid Expansion functions in that manner without a pandemic, helping ensure continued coverage for people with temporary, seasonal, or otherwise unstable employment, and Granite Staters with low incomes and unpredictable work hours. With about 50,000 people relying on Medicaid Expansion for their health coverage at any given point in the years leading up to the pandemic and enrollment rapidly increasing early in the pandemic, the program provides health coverage to fill a critical need for the state’s people and economy.
With a potential economic slowdown looming, Medicaid Expansion may become even more important in 2023 and 2024, rapidly providing health coverage to Granite Staters who lose employment. Medicaid Expansion, and the federal dollars it provides, can help New Hampshire residents weather financial uncertainty and have a more equitable and inclusive economy.
Appendix
The data presented below, provided by the New Hampshire Department of Health and Human Services, represent the benefits disbursed through Medicaid Expansion on a municipal basis. The columns show the number of residents enrolled in Medicaid Expansion by municipality as of August 1, 2022, the sum total number of months unique individuals were enrolled in the program by municipality during SFY 2022, and the number of dollars expended through Medicaid Expansion during SFY 2022 in service expenditure payments by municipality based on enrollee addresses. During SFY 2022, the federal government paid for 90 percent of service and administration costs.
The dollar values in the Payments to Providers column do not necessarily represent dollars expended within the boundaries of the municipality itself for services, but show the number of dollars used to provide these enrollees with services. For example, if an individual whose address is in Francestown were to receive care in a hospital in Nashua, the dollars would appear under Francestown in this table; the service expenditures may have taken place in Nashua, but the benefits were connected to a person who lives in Francestown. These figures are subject to revision following future adjustments to payments and include both the federal and non-federal shares.
These dollar figures have changed substantially from prior years in part due to two policy changes. First, with the transition of Medicaid Expansion in New Hampshire from the New Hampshire Health Protection Program to the New Hampshire Granite Advantage Health Care Program, enrollees who previously received assistance purchasing plans on the individual marketplace through the Premium Assistance Program were shifted to being enrolled in coverage through managed care organizations contracting with the State, which was a more cost-effective method of service delivery. Second, the federal Public Health Emergency’s continuous enrollment provisions have led to higher overall enrollment levels, as restrictions on disenrollment have been implemented by the federal government.[74]
Please see the resource PDF for the full appendix.
Endnotes
[1] For more information on Medicaid Expansion, see the Medicaid and CHIP Payment and Access Commission webpage Overview of the Affordable Care Act and Medicaid, the Kaiser Family Foundation’s September 2014 report Understanding How States Access the ACA Enhanced Medicaid Match Rates, and NHFPI’s 2018 Issue Brief Medicaid Expansion in New Hampshire and the State Senate’s Proposed Changes.
[2] See the federal poverty guidelines at the U.S. Department of Health and Human Services website HHS Poverty Guidelines for 2022, accessed December 20, 2022.
[3] Approximate populations from the U.S. Census Bureau’s American Community Survey One-Year Estimates for New Hampshire, Table S2701(see also Table 1701 for other poverty threshold levels). Federal poverty thresholds are typically calculated by the U.S. Census Bureau retrospectively for statistical purposes, whereas federal poverty guidelines are used to help determine program eligibility and a prospective; see the U.S. Department of Health and Human Services, 2020 Poverty Guidelines, U.S. Federal Poverty Guidelines Used to Determine Financial Eligibility for Certain Federal Programs webpage and the University of Wisconsin-Madison Institute for Research on Poverty’s What Are Poverty Thresholds And Poverty Guidelines? webpage for more information.
[4] For more information on Medicaid generally, see the Center on Budget and Policy Priorities Policy Basics: Introduction to Medicaid, updated April 2020.
[5] See Chapter 3, Laws of 2014. For more information about the beginning of the program, see the State of New Hampshire’s Information Statement for the General Obligation Capital Improvement Bonds 2020 Series A, page 42.
[6] See Chapter 13, Laws of 2016.
[7] See RSA 126-AA and NHFPI’s March 30, 2018 Issue Brief Medicaid Expansion in New Hampshire and the State Senate’s Proposed Changes.
[8] For more explanation of Medicaid Expansion’s history in New Hampshire, see NHFPI’s March 30, 2018 Issue Brief Medicaid Expansion in New Hampshire and the State Senate’s Proposed Changes, NHFPI’s May 10, 2018 blog post Senate Approves Medicaid Expansion Bill as Amended by the House, and the October 24, 2022 Final Report of the Commission to Evaluate the Effectiveness and Future of the New Hampshire Granite Advantage Health Care Program (SB 313, Chapter 342:1, Laws of 2018).
[9] Data from the New Hampshire Department of Health and Human Services December 2016 Caseload Report and from a December 12, 2016 New Hampshire Department of Health and Human Services presentation on the Premium Assistance Program, referenced in NHFPI’s March 2018 Issue Brief Medicaid Expansion in New Hampshire and the State Senate’s Proposed Changes.
[10] See NHFPI’s March 30, 2018 Issue Brief Medicaid Expansion in New Hampshire and the State Senate’s Proposed Changes. Enrollment data comparison made using the November 2017 New Hampshire Department of Health and Human Services Caseload Report.
[11] Figure for December 31, 2022 from the New Hampshire Department of Health and Human Services New Hampshire Medicaid Enrollment Demographic Trends and Geography report from January 4, 2023.
[12] Total enrollment figure provided by the New Hampshire Department of Health and Human Services on December 30, 2022.
[13] For more information on the responsiveness of Medicaid Expansion to recessions, see the Kaiser Family Foundation’s December 13, 2022 report Medicaid Enrollment among the Unemployed During the COVID-19 Pandemic and Beyond. See also the January 2017 Health Affairs research article Adults Are More Likely to Become Eligible For Medicaid During Future Recessions If Their State Expanded Medicaid and the Center on Budget and Policy Priorities July 2020 report States That Have Expanded Medicaid Are Better Positioned to Address COVID-19 and Recession.
[14] For more information related to irregular hours and turnover in lower-wage work, see NHFPI’s May 2019 Issue Brief Medicaid Work Requirements and Coverage Losses and NHFPI’s October 2019 Issue Brief The Potential Impacts of Proposed SNAP Eligibility and Work Requirement Changes on Food Insecurity.
[15] For turnover by industry, see the U.S. Bureau of Labor Statistics Table 16. Annual Total Separation Rates by Industry and Region, Not Seasonally Adjusted, accessed December 20, 2022. For New Hampshire data on employment by sector, see New Hampshire Employment Security’s Covered Employment and Wages annual averages for 2021.
[16] For enrollment data, see the New Hampshire Department of Health and Human Services October 6, 2022 report to the Joint Legislative Fiscal Committee, Granite Advantage Health Care Trust Fund, SFY 2022 Activities and Operations, FIS 22-375. For income and industry data, see NHFPI’s February 24, 2021 Fact Sheet Resource Inequities Across Counties and January 19, 2022 presentation New Hampshire Local Economy Indicators.
[17] Data provided by the New Hampshire Department of Health and Human Services via email on December 14, 2022. The data represent information available to the Department as of November 30, 2022. See the final endnote for more details.
[18] Medicaid Expansion enrollee race and ethnicity data provided by the New Hampshire Department of Health and Human Services on December 30, 2022. Comparison with the overall population used percentage breakdowns of race and ethnicity from the November 30, 2022 Medicaid Expansion enrollment and the 2020 Census counts for New Hampshire from the U.S. Census Bureau, Table P2. The category “American Indian and Alaska Native” title was changed to “Native American or Alaskan” in this analysis, and referred to as “Native American” in the text.
[19] Data collected from the U.S. Census Bureau’s American Community Survey, 5-Year Estimates from Table S2701.
[20] See NHFPI’s August 30, 2019 Issue Brief New Hampshire’s Workforce, Wages, and Economic Opportunity and September 4, 2020 Issue Brief Challenges Facing New Hampshire’s Workers and Economy During the COVID-19 Crisis.
[21] Data for New Hampshire and Maine collected from the U.S. Census Bureau’s American Community Survey, 5-Year Estimates from Table S2701.
[22] Data collected from the U.S. Census Bureau’s American Community Survey, 5-Year Estimates from Table S2701.
[23] Data collected from the U.S. Census Bureau’s American Community Survey, 5-Year Estimates from Table S2701.
[24] For more information, see the Center on Budget and Policy Priorities June 16, 2021 publication Medicaid Expansion: Frequently Asked Questions.
[25] See the New Hampshire Department of Health and Human Services October 6, 2022 report to the Joint Legislative Fiscal Committee, Granite Advantage Health Care Trust Fund, SFY 2022 Activities and Operations, FIS 22-375.
[26] See the New Hampshire Department of Health and Human Services October 6, 2022 report to the Joint Legislative Fiscal Committee, Granite Advantage Health Care Trust Fund, SFY 2022 Activities and Operations, FIS 22-375.
[27] For more information on the federal response to the COVID-19 pandemic, see NHFPI’s February 10, 2022 Issue Brief Public Benefit Navigators Can Help Granite Staters Access Federal Assistance and Support the Economy and April 14, 2020 Issue Brief The COVID-19 Crisis in New Hampshire: Initial Economic Impacts and Policy Responses. See also NHFPI’s December 6, 2022 presentation Federal Pandemic-Related Funding in New Hampshire: Impacts, Opportunities, and Benefits.
[28] For more information, see NHFPI’s June 30, 2022 blog post Thousands of Granite Staters Risk Losing Medicaid Health Coverage at the End of the Public Health Emergency. For the April 1, 2023 statutory end date to the connection between the federal Public Health Emergency and the continuous Medicaid enrollment requirement, see the Center on Budget and Policy Priorities December 21, 2022 blog post Year-End Bill Invests in Kids’ Health Coverage, Makes Tradeoffs in Area of Medicaid Continuous Coverage, Georgetown University Health Policy Institute’s December 20, 2022 post Unwinding Wednesday #15: Congress Proposes to End Medicaid Continuous Coverage Protection in Early 2023; Adds Transparency and Accountability Requirements, and the Utah Department of Health and Human Services web page Utah Medicaid, the Public Health Emergency, and Unwinding the Continuous Eligibility, accessed December 30, 2022.
[29] Enrollment data from the New Hampshire Department of Health and Human Services Caseload Reports for February 2020 and October 2022.
[30] Data provided by the New Hampshire Department of Health and Human Services on January 5, 2023.
[31] See the Kaiser Family Foundation’s May 10, 2022 report Fiscal and Enrollment Implications of Medicaid Continuous Coverage Requirement During and After the PHE Ends.
[32] For monthly employment statistics, see New Hampshire Employment Security’s GraniteStats portal. For information on employment income losses in New Hampshire, see NHFPI’s May 28, 2021 blog post Unemployment Insurance and the Continued Economic Recovery from the COVID-19 Crisis.
[33] See the New Hampshire Department of Health and Human Services October 6, 2022 report to the Joint Legislative Fiscal Committee, Granite Advantage Health Care Trust Fund, SFY 2022 Activities and Operations, FIS 22-375. For the April 1, 2023 statutory end date to the connection between the federal Public Health Emergency and the continuous Medicaid enrollment requirement, see the Center on Budget and Policy Priorities December 21, 2022 blog post Year-End Bill Invests in Kids’ Health Coverage, Makes Tradeoffs in Area of Medicaid Continuous Coverage, Georgetown University Health Policy Institute’s December 20, 2022 post Unwinding Wednesday #15: Congress Proposes to End Medicaid Continuous Coverage Protection in Early 2023; Adds Transparency and Accountability Requirements, and the Utah Department of Health and Human Services web page Utah Medicaid, the Public Health Emergency, and Unwinding the Continuous Eligibility, accessed December 30, 2022.
[34] For more information, see the New Hampshire Department of Health and Human Services, NH Medicaid (Medical Assistance) Eligibility for Children, accessed December 19, 2022. See also the U.S. Center for Medicare and Medicaid Services’ separate websites The Children’s Health Insurance Program (CHIP) and Children’s Health Insurance Program (CHIP), both accessed December 19, 2022.
[35] For the text of this study, see Health Affairs, Medicaid Expansion for Adults had Measurable ‘Welcome Mat’ Effects on Their Children, September 2017.
[36] See the December 2017 article Spillover Effects of Adult Medicaid Expansions on Children’s Use of Preventive Services in the journal Pediatrics from the American Academy of Pediatrics.
[37] Information provided by the New Hampshire Department of Health and Human Services on December 1, 2022, and retrieved from the State’s database on October 31, 2022.
[38] See the New Hampshire Department of Health and Human Services October 6, 2022 report to the Joint Legislative Fiscal Committee, Granite Advantage Health Care Trust Fund, SFY 2022 Activities and Operations, FIS 22-375.
[39] See the State of New Hampshire’s Information Statement for the General Obligation Capital Improvement Bonds 2022 Series A, page 52.
[40] See NHFPI’s May 10, 2018 blog post Senate Approves Medicaid Expansion Bill as Amended by the House and March 30, 2018 Issue Brief Medicaid Expansion in New Hampshire and the State Senate’s Proposed Changes.
[41] NHFPI calculations based on reported program expenditures in the March 2019 State of New Hampshire’s Information Statement, page 49 for bond purchasers, as well as the March 2022 Information Statement, page 51. Medicaid match rates used as provided by the Kaiser Family Foundation’s September 2014 report Understanding How States Access the ACA Enhanced Medicaid Match Rates.
[42] See the New Hampshire Department of Health and Human Services October 6, 2022 report to the Joint Legislative Fiscal Committee, Granite Advantage Health Care Trust Fund, SFY 2022 Activities and Operations, FIS 22-375.
[43] For more information, see NHFPI’s March 30, 2018 Issue Brief Medicaid Expansion in New Hampshire and the State Senate’s Proposed Changes and December 20, 2019 Issue Brief The State Budget for Fiscal Years 2020 and 2021. For the Medicaid Enhancement Tax’s inclusion in the revenue supporting the New Hampshire Granite Advantage Health Care Trust Fund, see RSA 126-AA:3, I(f).
[44] Data collected from the State of New Hampshire’s Information Statement for the General Obligation Capital Improvement Bonds 2022 Series A, page 51, and the New Hampshire Department of Health and Human Services October 6, 2022 report to the Joint Legislative Fiscal Committee, Granite Advantage Health Care Trust Fund, SFY 2022 Activities and Operations, FIS 22-375. Figures confirmed by the New Hampshire Department of Health and Human Services via email. All other Insurance Premium Tax revenues support the General Fund.
[45] See the New Hampshire Department of Health and Human Services October 6, 2022 report to the Joint Legislative Fiscal Committee, Granite Advantage Health Care Trust Fund, SFY 2022 Activities and Operations, FIS 22-375.
[46] See RSA 126-AA:3, I. Notably, key long-term services and supports are funded by counties and nursing facilities, and hospitals make a substantial contribution to Medicaid funding through the Medicaid Enhancement Tax. See NHFPI’s July 18, 2022 publication Long-Term Services and Supports in New Hampshire: A Review of the State’s Medicaid Funding for Older Adults and Adults with Physical Disabilities, page 21, for more details.
[47] See NHFPI’s February 2017 resource Building the Budget, page 12.
[48] See Chapter 342, Laws of 2018, and NHFPI’s February 2017 resource Building the Budget, page 18.
[49] See NHFPI’s July 18, 2022 publication Long-Term Services and Supports in New Hampshire: A Review of the State’s Medicaid Funding for Older Adults and Adults with Physical Disabilities, page 21, for more details.
[50] See the Commonwealth Fund’s May 5, 2020 report, The Impact of Medicaid Expansion on States’ Budgets, Appendix B.
[51] For more information, see the State of New Hampshire’s Information Statement for the General Obligation Capital Improvement Bonds 2022 Series A, pages 24 and 55.
[52] NHFPI calculations based on data provided by the New Hampshire Hospital Association on January 11, 2023.
[53] Data provided by the New Hampshire Department of Corrections on November 29, 2022.
[54] See the Commonwealth Fund’s May 5, 2020 report, The Impact of Medicaid Expansion on States’ Budgets.
[55] See the Commonwealth Fund’s May 5, 2020 report, The Impact of Medicaid Expansion on States’ Budgets.
[56] See the Commonwealth Fund’s May 5, 2020 report, The Impact of Medicaid Expansion on States’ Budgets and Manatt Health’s April 2021 analysis Assessing the Fiscal Impact of Medicaid Expansion Following the Enactment of the American Rescue Plan Act in 2021.
[57] See the Commonwealth Fund’s May 5, 2020 report, The Impact of Medicaid Expansion on States’ Budgets.
[58] See the University of Montana’s Bureau of Business and Economic Research January 2019 report The Economic Impact of Medicaid Expansion in Montana: Updated Findings and the Commonwealth Fund’s May 5, 2020 report, The Impact of Medicaid Expansion on States’ Budgets.
[59] See the Commonwealth Fund’s May 5, 2020 report, The Impact of Medicaid Expansion on States’ Budgets.
[60] See The Hilltop Institute of the University of Maryland, Baltimore County at The Economic Impact of Medicaid Expansion in Mississippi, 2023-2028.
[61] This two-phase literature review from the Kaiser Family Foundation includes summaries for the March 17, 2020, The Effects of Medicaid Expansion under the ACA: Studies from January 2014 to January 2020, and updated summary graphics from the May 6, 2021, Building on the Evidence Base: Studies on the Effects of Medicaid Expansion, February 2020 to March 2021, Appendix A.
[62] For the analysis of relevant studies from 2020 and early 2021, see the Kaiser Family Foundation’s May 6, 2021 report Building on the Evidence Base: Studies on the Effects of Medicaid Expansion, February 2020 to March 2021, pages 5-7. For the 2018 study specific to infant mortality, see the Center on Budget and Policy Priorities June 16, 2021 publication Medicaid Expansion: Frequently Asked Questions.
[63] This summary of health impacts was drawn from the Kaiser Family Foundation’s analysis from March 17, 2020, The Effects of Medicaid Expansion under the ACA: Studies from January 2014 to January 2020, pages 8-11, and from May 6, 2021, Building on the Evidence Base: Studies on the Effects of Medicaid Expansion, February 2020 to March 2021, pages 8-10.
[64] See the discussions of rural and small hospital finances in the March 17, 2020 Kaiser Family Foundation report, The Effects of Medicaid Expansion under the ACA: Studies from January 2014 to January 2020, page 18, and the May 6, 2021 follow-up report, Building on the Evidence Base: Studies on the Effects of Medicaid Expansion, February 2020 to March 2021, pages 9-10.
[65] NHFPI calculations based on reported program expenditures in the March 2019 State of New Hampshire’s Information Statement, page 49 for bond purchasers, as well as the March 2022 Information Statement, page 51. Medicaid match rates used as provided by the Kaiser Family Foundation’s September 2014 report Understanding How States Access the ACA Enhanced Medicaid Match Rates.
[66] This projection was published in the October 24, 2022 Final Report of the Commission to Evaluate the Effectiveness and Future of the New Hampshire Granite Advantage Health Care Program (SB 313, Chapter 342:1, Laws of 2018).
[67] For more on the economic multipliers of federal programs, see NHFPI’s February 2022 Issue Brief Public Benefit Navigators Can Help Granite Staters Access Federal Assistance and Support the Economy.
[68] For relevant research, see the journal Health Services Research, The Effect of Rural Hospital Closures on Community Economic Health, April 2006, as well as The Economic Effects of Rural Hospital Closures, June 2022 and Changes in Economic Outcomes Before and After Rural Hospital Closures in the United States: A Difference-in-Differences Study, October 2022. Relevant research also includes SSRN’s Rural Hospital Closures and Local Economic Decline, March 2021.
[69] For the summaries of different types of economic impacts, see the Kaiser Family Foundation’s May 6, 2021 report, Building on the Evidence Base: Studies on the Effects of Medicaid Expansion, February 2020 to March 2021, Appendix A.
[70] For more details on the economic and employment impacts found in the literature review, the Kaiser Family Foundation’s May 6, 2021 report Building on the Evidence Base: Studies on the Effects of Medicaid Expansion, February 2020 to March 2021, pages 19-20.
[71] See the Ohio survey results in the Ohio Department of Medicaid’s August 21, 2018 report Ohio Medicaid Expansion Assessment.
[72] For more details on this analysis, which uses a model from Regional Economic Models, Inc., see The Commonwealth Fund, The Economic and Employment Effects of Medicaid Expansion Under the American Rescue Plan, May 20, 2021.
[73] For more details, see The Hilltop Institute’s January 2022 publication The Economic Impact of Medicaid Expansion in Mississippi, 2023-2028: Technical Report, page 38.
[74] Payment and member month data provided by the New Hampshire Department of Health and Human Services via email on December 14, 2022. The data represent information available to the Department as of November 30, 2022. Data from municipalities with fewer than five average enrollees were suppressed by the Department due to privacy concerns. In prior releases of these data, the Department has tracked the home municipality of an enrollee based on their addresses at the first of the month, and provider payments have included both fee-for-service payments, prior to the switch from the New Hampshire Health Protection Program to the New Hampshire Granite Advantage Health Care Program, and health plan capitation payments. The Department has also not included enrollees who are being treated at an out-of-state facility, including those who have moved or in the process of moving; the Department reported in 2018 that this number is typically about ten people. These figures are subject to revision, including based potential on future adjustments to expenditure totals for past procedures and care.